INJURIES IN MINES AND OTHER EXPLOSIVES
Types of injuries, mechanism and first aid to mines and other explosives
The pattern of injuries caused by mines and other explosive devices is extremely complex. It depends on the structure of the explosive, the amount of explosives, the method of administration, as well as the distance between the accident and the explosive wave. For this reason, injuries caused by an explosive device require a unique triage procedure, diagnosis, and management of the injured.
Explosives are categorized as strong (high-order explosives, HE) and weak (low-order explosives, LE). Mines, UXO and similar devices are classified in the category of strong explosives, while gunpowder and petroleum-based bombs such as the Molotov cocktail are classified in the category of weak explosives. A special category consists of improvised explosive devices , which can be: HE, LE or a combination of both. Knowing the structure of an explosive device can predict the pattern of injuries and provide more effective assistance to the casualty.
Blast injuries
Injuries caused by explosives are referred to as blast injuries . First of all, it is necessary to distinguish between the terms shock wave and shock wind. A shock wave is a physical component that results from the release of high pressure after the explosive is activated, while a shock wind is a result of a force manifested by the flow of an air stream with extreme thermal action. The shock wave is characteristic only for HPPs, while the shock wind is characteristic for both HPPs and LEs.
Considering the differences in the mechanisms of action of HPPs and LEs, separate classifications of injury patterns were performed. Injuries caused by LE are classified as: ballistic (fragmentation), injuries caused by gusts of wind and thermal. There is a descriptive difference in certain categories in relation to HPPs. Injuries caused by HPPs according to the mechanism of action of the explosive device (Table 1) are classified into four categories:
- Primary category is a set of injuries that are accompanied by anatomical and physiological changes, and occur as a result of the shock wave of an explosive device. Injuries of this category lead to the emergence of the so-called. blast syndrome .
- Secondary category is a set of injuries resulting from flying debris and explosive fragments
- Tertiary category is a set of injuries that occur as a result of contact of the casualty with the ground after rejection by gusts of wind .
- The Quaternary category is a set of injuries and complications that do not occur as a result of the mechanisms of the previous three categories. It is also a complication of the victim's current condition.
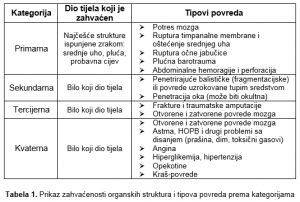
Table 1. Overview of the involvement of organic structures and types of injuries by category
Triage procedure for blast injuries and access to the casualty
If there are several injured at the scene of the accident, the triage procedure is performed according to the STaRT algorithm ( Simple-Triage-and-Rapid-Treatment ), which includes an assessment of the ability to move, states of consciousness, respiration, and pulse. The red rectangle represents the casualties who are in acute vital danger , the yellow rectangle represents those who are severely injured , and the green rectangle represents those who are slightly injured . The black rectangle represents casualties who have no chance of survival .
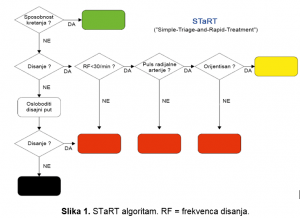
Figure 1. STaRT algorithm. RF = respiratory rate.
The evaluation of casualties is performed according to the ABCDE scheme of the critical patient, which at the beginning of the examination implies grading critical bleeding as a key aspect for further treatment of the casualty, as evidenced by available studies from the military sector. In addition, a potential cervical spine injury is evaluated. This structured and priority-oriented assessment and remediation needs to be implemented in one to two minutes according to the following steps:
- A - Airway patency : Clean the airway and immobilize the cervical spine if there is a suspicion of injury (cervical orthosis) )
- B - Breathing
- C - Circulation - Critical bleeding In the event of life-threatening bleeding, it should be stopped immediately.
- D - Disability
- E - Exposure
Identification and first aid for primary injuries
Lung and abdominal wall barotrauma are associated with a high mortality rate, with lung barotrauma being among the most common injuries in survivors.
Any organ system can be affected by blast injuries, and up to 10% of all survivors have significant eye injuries . Such injuries are mostly characterized by initial discomfort and can be present for days, weeks and months. Symptoms include eye pain or irritation, altered visual acuity, bruising, and swelling of the eyeball.
Brain injuries after a shock wave can range from concussions to mild traumatic brain injuries (MTBI). Brain injuries should be suspected if the casualty develops fatigue, decreased concentration, slowness, depression, anxiety, insomnia, or other associated problems. Concussion and acute stress disorder have similar characteristics.
Pulmonary barotrauma is a direct result of the action of the shock wave. It is the most common fatal primary injury among survivors. Signs of pulmonary barotrauma are usually present during the initial evaluation of injuries, but may also occur 48 hours after the explosion. It is characterized by a clinical triad of symptoms: apnea (cessation of breathing) , bradycardia (slow pulse) , hypotension (low blood pressure). Scattered petechiae (spotting) and confluent bleeding appear on the chest. Pulmonary barotrauma should be suspected in anyone who has a respiratory disorder, bloody cough and chest pain, and has previously been exposed to a shock wave.
Blast injuries to the hearing system can cause significant consequences and are easy to overlook. The injury depends on the orientation of the ear towards the explosion. Among the most common are injuries to the middle ear (perforation of the tympanic membrane). Signs of an ear injury are present during the initial evaluation and should be suspected in anyone with a hearing impairment, tinnitus, ear pain, dizziness, bleeding from the external auditory canal, leakage of turbid fluid from the ear.
Air-filled organs of the abdominal cavity , such as the organs of the digestive tract, are the least resistant to the action of a shock wave. Such action can cause immediate perforation of the intestine, bleeding (from punctate to large), clefts of solid organs, clefts of the testicles. Blast injuries of the abdominal organs should be suspected in anyone with abdominal pain, nausea, vomiting, vomiting of blood, rectal pain, false urges to stool, pain in the testicles, hard abdominal wall.
Injuries to the eye and ear caused by this mechanism of action do not represent life-threatening injuries, while brain injuries at the time of rehabilitation have no significant consequences. Barotrauma of the lungs and abdominal cavity is manifested by various mechanisms of internal bleeding, and in the case of barotrauma of the lungs, there is also the possibility of air embolism , and these injuries are life-threatening. For this reason, the casualty should be placed during transport in a mild Trendelenburg position (internal bleeding in the abdominal cavity) and a Durant maneuver should be applied (left lateral pressure ulcer with low head).
Identification and first aid for secondary and tertiary injuries
The secondary and tertiary categories of injuries require the simultaneous approach of a rescuer. When it comes to landmines and explosives whose action is based on direct contact with the casualty, injuries of the secondary category are predominantly dominant over injuries of the tertiary category. Due to the penetration of a large number of fragments of explosives into the lower extremities, they are most often amputated, and it is necessary to approach the victim according to the scheme of the critical patient. In the case of smaller amputations, the manipulation is performed with sterile gauze, while the manipulation of larger amputations is performed with sterile materials of larger dimensions, such as a triangular scarf. We put the amputate in a bag, and then together with the bag in a bag with ice. The following information is entered on the bag: name and surname of the victim, date of birth, body part of the amputee and the time after the amputation was completed. Other areas indicating fragment penetration should be treated as a region-specific injury caused by a foreign body.
Fractures suffered by the victim by the mechanisms of the tertiary category of injuries should be treated according to the first aid protocols.
Identification and first aid for certain quaternary injuries
The range of quaternary category injuries is extremely wide, and requires a multidisciplinary approach. For this reason, certain conditions and injuries will be described below, which are among the most common, common to most explosive devices and require prompt action by rescuers.
Burns are a type of injury to the skin and other tissues caused by heat. When burns, in addition to local action, also cause indirect changes in the whole organism, then it is a burn disease . Explosives filled with HPP explosives cause burns of the thermal type which are a consequence of the thermal action of the means itself, the secondary fire, as well as the thermal action of the fragments of the explosive. Explosives based on phosphorus and other war poisons from the group of blisters cause a special group of burns of the chemical type . Minor and superficial burns are overcome by compensatory mechanisms, while deep burns, which cover more than 20% of the skin surface in adults and more than 10% of the skin surface in children, can lead to the development of burn shock , if not taken. timely measures. Burns are classified according to the percentage and depth of the affected area (four degrees). First degree burns are characterized by redness of the burnt surface , secondary appearance of bulla (burn blisters, blisters), tertiary discoloration of the burnt surface (from pale to dark) and the appearance of eshara (hard skins), while the fourth degree is characterized by carbonization (charring). The percentage of surface coverage is determined by the Wallace rule of the ninth (Figure 2) and is based on the following percentage distribution:
- Head and neck area: 9%
- Hull front area: 2 × 9% = 18%
- Back area: 2 × 9% = 18%
- Hand area: 9%
- Foot area: 2 × 9% = 18%
- Genital region (external): 1%
- Isolated hand burns: 1%
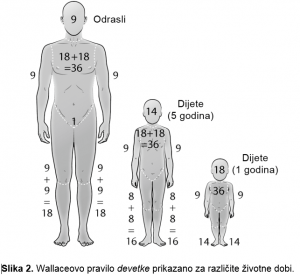
Figure 2. Wallace's rule of nine is shown for different ages.
When approaching an injured person with burns, it is necessary to exclude the possibility of inhalation burns caused by inhaling smoke and hot air. Respiratory burns can disrupt the vital parameters of the injured person, and they should be suspected if the injured person has the following characteristics: burnt eyebrows and nose hair, burns in the mouth, black cough, hoarseness. In this case, it is necessary to place the injured person in a sitting position, and cool the chest with a damp gauze, sponge or some other improvised means that could be used to apply this procedure. During the orientation examination of the injured person, it is necessary to roughly determine the percentage of surface involvement of burns as well as the dominant type of burns according to the depth of involvement, and to treat them according to standard first aid procedures.
Crash injuries are mechanical injuries that occur when large parts of the body (extremities, areas of large muscle mass) are exposed to prolonged and strong pressure, leading to disruption or disruption of blood flow. They occur in various situations such as: earthquakes, accidents in mines, traffic accidents, etc. Explosive devices do not cause them directly but indirectly, if their activation occurs, e.g. in a building, due to destabilization and the fall of larger structures on the casualty. Apart from indoors, it is also possible for them to occur in the open (fall of parts of the tree after the explosion, landslide of larger pieces of rock, etc.). The danger for the injured person in case of a crash injury is the occurrence of a crash syndrome , which is a life-threatening condition for the injured person, and the conditions for its occurrence are directly proportional to the length of exposure to the pressure of a heavy object. Crash syndrome is based on systemic changes in the casualty, which are the result of traumatic muscle breakdown, which in most cases leads to shock and kidney failure . The approach to the injured is based on determining the length of exposure to the pressure of a heavy object, as well as on preventing the development of crash syndrome. If the exposure lasted less than 15 minutes (exposure threshold varies from author to author), it is necessary to remove the object as soon as possible, and access standard first aid protocols and repair the resulting injuries (bleeding, fracture, etc. pristupa) ). If the exposure lasted longer than 15 minutes, the item must not be removed until the arrival of the emergency medical team. During this time, it is necessary to repair other injuries and monitor the vital parameters of the victim. If the access of the emergency medical care team is prevented, the object must be removed, and a tourniquet is placed on the affected limb above the site of pressure, in order to prevent and slow down the occurrence of crash syndrome. After setting up the tourniquet, it is necessary to enable the injured to provide emergency medical care in the shortest possible time interval.
Inhalation of toxic gases poses a risk to both the casualty and the team approaching the casualty. Significant use of explosives based on white phosphorus was noticed on the territory of Bosnia and Herzegovina, and its characteristics and action will be described below, as well as the approach to the victim. Rescue can be accessed only by a unit composed of individuals certified to rescue casualties from the area of action of war poisons, and for other rescue teams and individuals is content that is purely informative, which is a measure of prevention, protection and self-protection of rescue teams. White phosphorus is a solid, transparent substance that varies from white to yellow, and darkens when exposed to light. It is very reactive and self-igniting if exposed to air. In the past, it was used to make pesticides and fireworks, and later it was also used for military purposes (photography).

Photo. Application of white phosphorus on the territory of Syria. Source: snopes.com
White phosphorus can contaminate soil and water if applied in a solid state. It can be recognized by its scent, which is reminiscent of the smell of burnt matches, garlic , and is extremely sour and irritating . Of course, the characteristics of its odor may not necessarily be applied to assess a potentially contaminated area. Toxic fumes caused by its combustion (phosphorus oxides) are extremely irritating and lead to systemic manifestations, which are characterized by three phases that take place in a short period after exposure and manifest their effects over several days. The initial phase is characterized by the possibility of extremely severe shock, which can result in death, and if the victim survives, the consequences are possible in the form of multiple organic failure, damage to the nervous system , which ultimately leading to a fatal outcome. White phosphorus enters the human body by inhalation, ingestion and skin contact, and it is not known whether contact with the eyes can lead to systemic manifestations. Access to the injured person strictly depends on the assessment of a person who knows the action of explosives based on war poisons, as well as protocols for the protection and self-protection of individuals in contaminated areas. Self-protection measures are taken through decontamination of the rescuer who approaches the injured person and the use of protective equipment. Protective equipment is applied through four levels (A, B, C, D), and the application is based on the protection of the skin (suits resistant to the chemical action of the substance) and the respiratory system, the so-called. air purifier ( PAPR = Powered Air Purifying Respirators ) (Figure). If the safety conditions are met, the casualty can be approached.

Photo. Examples of protective equipment and PAPR.
Decontamination of the injured person is the first procedure and is based on the transport of the injured person through the decontamination corridor from the contaminated zone to the so-called safe zone , protocols for removing his clothes, as well as decontaminating his skin. After the absence of shock and the stability of the vital parameters of the victim are determined, an orientation examination is performed, during which the intensity of injuries caused by white phosphorus particles and the action of toxic fumes is determined. There is no antidote for white phosphorus intoxication, which is an aggravating circumstance for the victim. The victim should rinse their eyes with chilled water for at least 15 minutes , and then cover them with a damp gauze or cloth to prevent reactivation of phosphorus. Areas of burns caused by white phosphorus should be kept moist until the particles can be squeezed out or removed. The water temperature that maintains the humidity of the burned area is about 40 ° C , which is close to the melting point of phosphorus (44.15 ° C) and thus facilitates its removal. If water sources as well as equipment that would achieve the specified temperature are not available, the alternative is achieved by using urine , which is physiologically sterile and has an approximate temperature. Some authors also mention the use of cold water for the purpose of removing particles, where there is a risk of hypothermia (hypothermia). When removal cannot be performed by extrusion, removal is performed using forceps (medical forceps), and as a last resort, if it is not possible to remove phosphorus particles even using forceps, 5-15% is applied. > copper sulphate solution , which does not allow phosphorus to burn. After removing the particles, the standard first aid procedures for repairing larger burns are approached, and the injured person is transported to the nearest area, where he can be given urgent medical help. Deviation from any segment of the protocol significantly increases the security risk of all present.
Dr Adi Osmanbegović